Not a Happy Fraction of a Man
Phantom limbs and the imagined security of the body
Gaby Wood
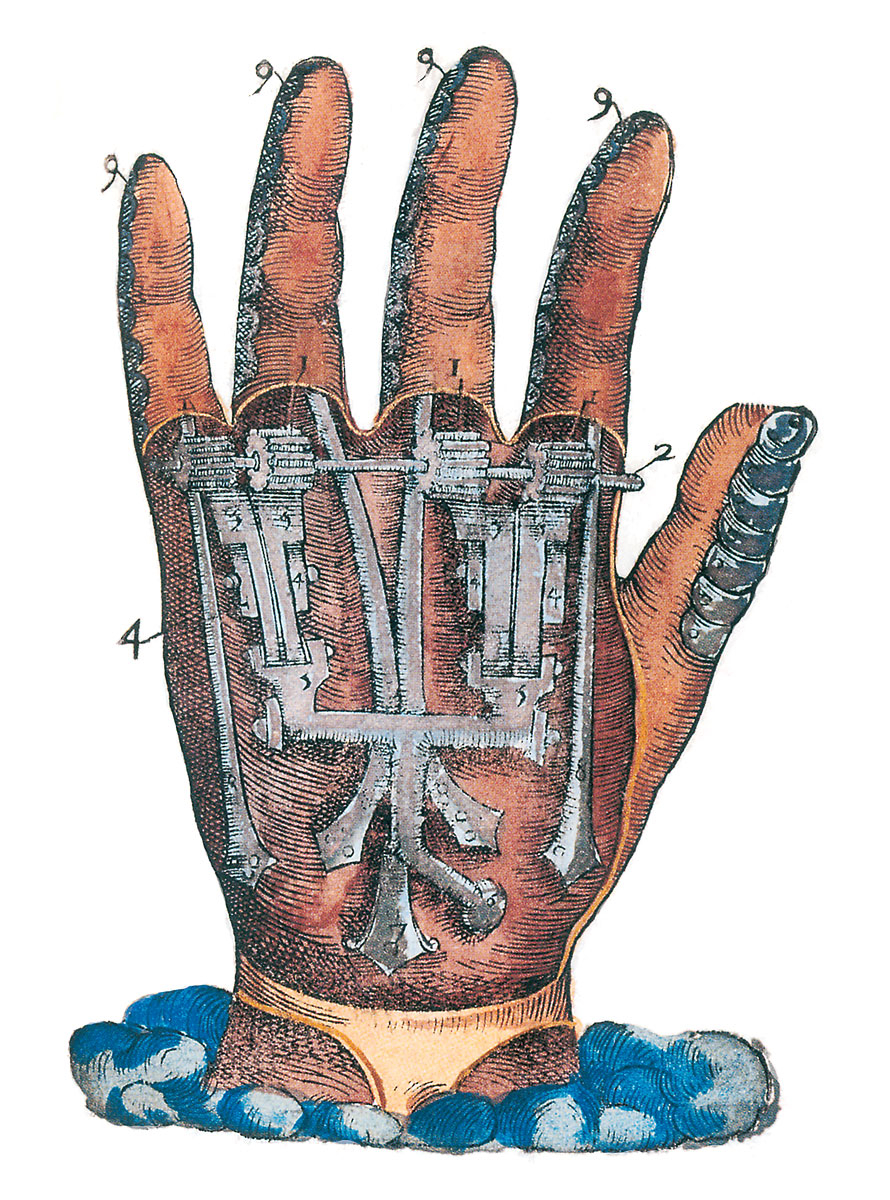
In the mid-sixteenth century, the great French surgeon Ambroise Paré discovered what he described as a “strange and grievous fact.” As surgeon to François I, Paré had accompanied the king on military campaigns of exceptional brutality. Thousands of French cavalrymen were killed and wounded by arquebuses, precursors of the musket that looked like small handheld cannons and could blast even the most heavily armored bodies to pieces. Paré treated the wounds made by these weapons with turpentine and rose water, and he pioneered a safer method of amputation. But while creating his signature tourniquets, he found he could not tie up arteries without bruising nerves as well. The “strange and grievous fact” that arose as a consequence was that men who had lost their limbs felt the limbs to be still there. Not only did the patients imagine them, but they sometimes felt pain in these limbs, tried to walk on their non-existent legs, or reach for objects with a missing arm. Paré designed artificial body parts for his amputees, beautiful constructions to be made in metal by armorers, but he could do nothing for these strange configurations of the mind.
Paré was the first to set down the phenomenon in writing; centuries later, in the course of another war, the writer and neurologist Silas Weir Mitchell gave it a name. He said his patients were suffering from “phantom limbs”—since these “vivid hallucinations” were in fact a form of haunting. “Nearly every man who loses a limb,” Mitchell wrote, “carries about with him a constant or inconstant phantom of the missing member, a sensory ghost of that much of himself.”
Mitchell was thirty-three years old when he became a contract surgeon for the Union Army during the American Civil War, a conflict that saw unprecedented numbers of men made limbless. His arrival at Gettysburg just after the famous battle made a deep impression on him, and ensured that he would despise war to the end of his days. There were 27,000 wounded to be cared for when he got there. Mitchell said he “smelt nine hundred smells,” and later spoke of “the dead Confederates ... with arms and legs in rigid extension—a most horrible memory.” Walt Whitman, who spent the war working in a field hospital as a volunteer nurse, described seeing the remains of countless surgeries. There was, he wrote, “a heap of feet, legs, arms and human fragments, a full load for a one-horse cart.”
But amputation was safer and less painful than it had been before—ether and chloroform were now used, and the longer operating time these allowed made for more effective stumps. Mitchell was eventually placed in charge of Turner’s Lane Hospital in Philadelphia, which received a large number of nervous cases, and he made his reputation on the research he conducted there into nerve injuries and gunshot wounds. He identified the condition that was to become known as “shell shock,” but was occupied more specifically with the thousands of amputees who populated the Philadelphia “Stump Hospital.”
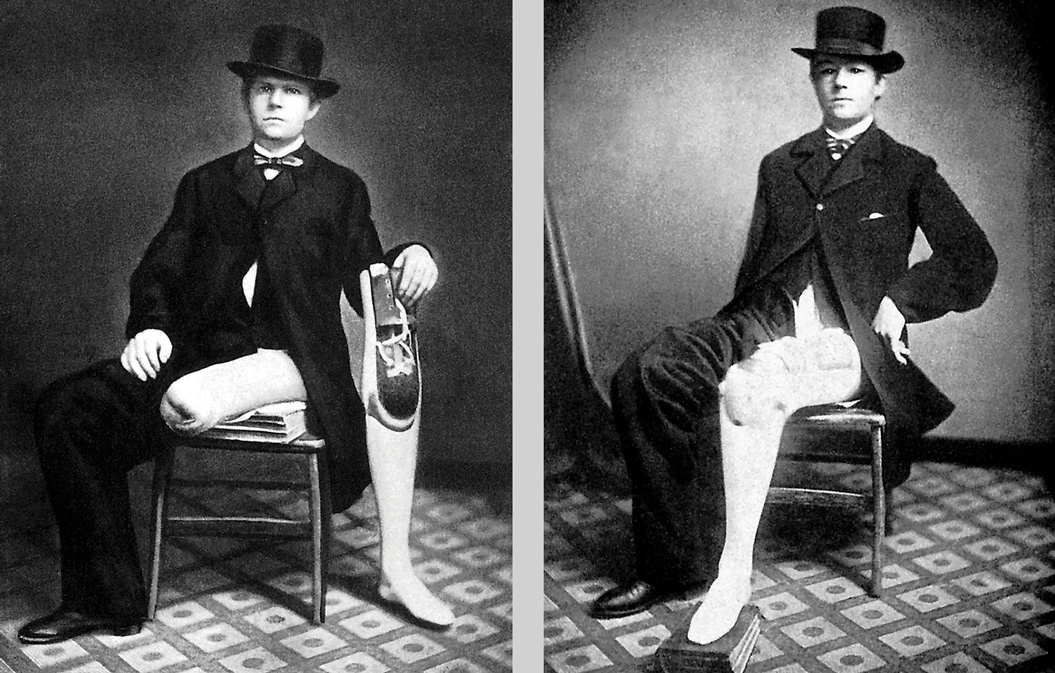
Writing in a popular magazine in 1871, Mitchell estimated that about 15,000 men across the country had lost an arm or a leg during the war, though only 6,075 of them had been supplied with artificial limbs so far. (In fact, there were around twice that many amputations conducted in the Union Army alone. And in 1862, a year after the start of the war, the American government officially began providing funding for one free prosthesis per amputation for soldiers and sailors.) The sheer number of patients Mitchell saw allowed him to observe the “strange and startling phenomena” associated with phantom limbs, a form of neuralgia he concluded must stem from inflamed or otherwise damaged nerves in the amputee’s stump. Far from being an unusual condition, it was one Mitchell found to be present in all but five percent of cases, and he could offer no explanation for the exceptions. He saw one man who was so sure of his missing arm that he went riding and used the lost hand to grasp the reins, causing an accident. Another thought he had punched someone, but realized he had taken aim with his phantom fist. A third complained of chronic nausea, since every time he sat down to eat he tried to pick up a fork and felt sick at his failure.
“There is something almost tragical, something ghastly,” Mitchell wrote, “in the notion of these thousands of spirit limbs haunting as many good soldiers.” Indeed, in many cases he found a curious version of the commonly held belief about ghosts—that people who have died violently are condemned to roam the earth in the condition in which they have been left. Some amputees in Mitchell’s care found their phantom limbs stuck in the position in which they had last felt them; the last real sensation in the limb remained forever, so that a phantom hand might be paralyzed with the thumb cutting into the palm, or the fingers rigid in agony.
In the course of his article, Mitchell mentioned another, which had been published anonymously years earlier in the Atlantic Monthly. It was a “humorous sketch,” a “jeu d’esprit,” he said, whose fictional protagonist—a man who had lost all his limbs during the Civil War—was so realistically drawn that a number of readers had erroneously sent donations to him at the Stump Hospital. Mitchell portrayed this earlier article as an irresponsible piece of writing, and claimed that his own would describe, correctly and scientifically, the experiences of those haunted by phantom limbs.
As it happens, however, Mitchell was only correcting himself. “The Case of George Dedlow,” as the Atlantic Monthly article was called, was Mitchell’s first attempt at writing fiction—a second career in which he was to excel. Far from being funny, it was a portrait of a man who had lost everything, including his sense of self, and it clearly succeeded in eliciting a good deal of sympathy from a general public who had until then believed, along with most doctors, that phantom limbs were all in the mind.
In the story, Dedlow describes himself as “not a happy fraction of a man.” His arms are blown off, and later in the war he loses both legs: “Against all chances I recovered, to find myself a useless torso.” He still feels his missing legs, however, and explains the medical reasons for this in layman’s terms: the nerve, which once led to the extremity and remains in the stump, “is like a bell-wire. You may pull it at any part of its course, and thus ring the bell as well as if you pulled at the end of the wire.”
Gradually, Dedlow experiences a psychic loss more dramatic than the physical loss of his limbs; as he lies in hospital, motionless and bed-bound, he feels his identity beginning to erode. He wonders “how much a man might lose and yet live,” since “to lose any part must lessen his sense of his own existence.” Dedlow is so bewildered by his loss of self that he feels “like asking someone constantly if I were really George Dedlow or not. ... At times the conviction of my want of being myself was overwhelming and most painful.”
The story ends with a visit Dedlow makes to a spirit medium, who summons his amputated legs from the afterlife. They identify themselves—rapping on the table—by two numbers: their catalogue codes from the United States Army Medical Museum. Dedlow is, he says, “reindividualized,” returned to himself, and so entranced by this spirit communication that he walks across the room on invisible legs, astonishing everyone with his miraculous behavior, before sinking feebly to the floor.
Mitchell’s short story was an exaggeration, of course, but it encapsulated a number of things connected with phantom limbs, and by extension, with the artificial limbs designed to replace them. The limbs are called phantoms because they are felt manifestations of something that does not physically exist—they are, in Mitchell’s words, “sensory hallucinations.” But they are also phantoms in their connection to the spirit world—produced, like the ghosts of the dead, in response to a loss. No matter what the neurological explanation for the phenomenon, phantom limbs are a form of mourning—the body’s, or the mind’s, way of making up for what has gone. Whenever surgeons performed repeated amputations, shortening the stump incrementally in an attempt to rid the sufferer of his delusion, the phantom would return with a vengeance, reasserting itself with every loss. So much is the phantom limb connected to the notion of an afterlife that Lord Nelson, on losing his right arm in battle, believed the phantom arm that replaced it to be “direct evidence for the existence of the soul.” If an arm could survive amputation, he proclaimed, why should an entire person not live on after death?
In a book called The Phantom Limb Phenomenon (1978), Douglas B. Price and Neil J. Twombly collected a number of accounts, from the tenth century onwards, of the miraculous restoration of lost body parts, a common folkloric trope that they argue is related to the experience of phantom limbs. After all, is a person who believes his lost limb to have been restored to him by a miracle so different from the person who, sometimes weeks or years after the wound has healed, becomes conscious of his missing limb? Mitchell reported one case in which a patient had no phantom limb at all until two years after the amputation, when a mild electrical current was passed through his body, at which point he grasped at thin air and shouted in pain: “Oh, the hand! The hand!” “No resurrection of the dead, no answer of a summoned spirit, could have been more startling,” Mitchell wrote. Might the religious and medical narratives be analogous?
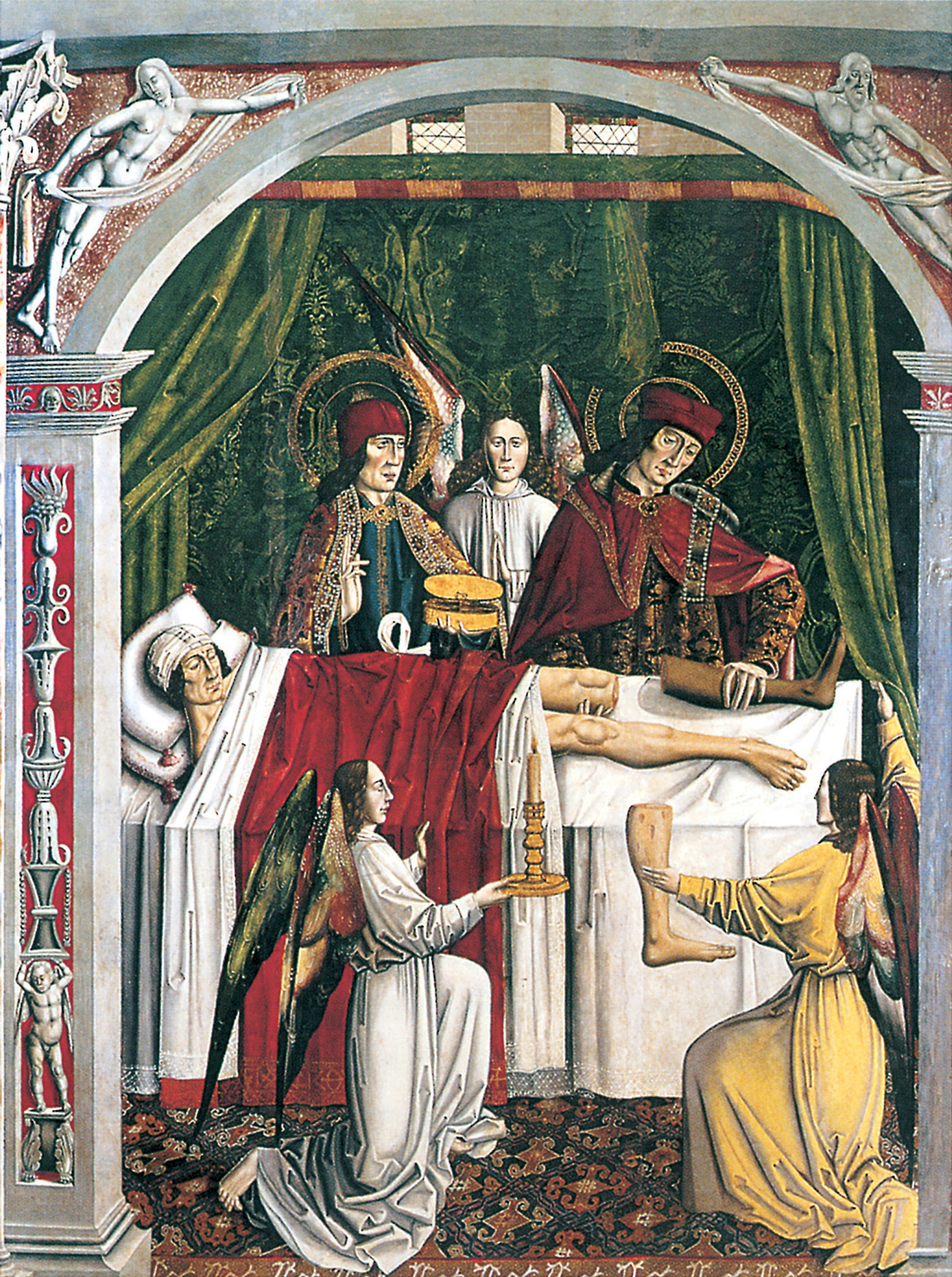
One of the miracle tales, so famous as to have been painted repeatedly (in one depiction by Fra Angelico) concerns a leg transplant performed by two saints, Cosmas and Damian. Summoned by Pope Felix to help a man whose leg is cancerous, Cosmas and Damian cut off the man’s leg. But “where,” they ask, “shall we get flesh to fill up this void?” The angel Raphael appears to them and tells them that an Ethiopian has just been buried in a graveyard nearby. They are to dig up his body and cut off his leg. Then, the angel instructs them, on the day of the resurrection, they must orchestrate a swap. The saints do as they have been told, and sure enough, once the exchange has been effected, they see that each leg has become attached, by some miracle, to the person by whom they had lain it. The dead Moor has one white leg, and the man who had cancer awakes to find his leg fully functioning, though it is clearly, by its color, someone else’s.
“Putting then a candle nearby,” reads one account of this awakening, “when he saw nothing wrong in the leg, he thought that he was not who he was, but someone else.” Another account, a poem printed by William Caxton in 1483, reads as follows: “and when the seke man a woke/ and felte no payne/ he put forthe his honde/ and felte his legge withoute hurte/ And thenne tooke a Candel/ and sawe wel that it was not his thye/ but that hit was a nother/ And when he was wel come to hym self/ he sprange oute of his bedde for joye.”
This story is not unlike that of George Dedlow needing to be reminded, as his physical self becomes more alien to him, that he is who he thinks he is. But unlike George Dedlow, this man does not recognize himself because he has acquired a body part that is foreign to him—something new has been added. In that respect, he is more like a patient described by the contemporary neurologist Oliver Sacks. “The man who fell out of bed,” as Sacks calls him, suffers from a delusion that is a reversal of a phantom limb: he thinks his own leg is someone else’s, stolen from the dissecting room and placed under the sheets of his hospital bed as a joke. But when he tries to throw the leg out of the bed the rest of his body goes with it, since it is in fact his own, and still attached. He ends up on the floor, and can’t get up, because the leg he sees is so seemingly separate as to be of no use to him. He can’t make it move because he is so disgusted by it that he is unable to accept it. He is horrified by the leg, calls it “ghastly,” “uncanny,” “a counterfeit,” and expresses some astonishment at the idea that anyone should have gone to such lengths as to manufacture “a facsimile.”
In the story of the saintly transplant, it is no accident that the leg donor is a “Moor.” The transplant is considered a miracle because the impossible has been performed: the donor was initially dead (so some form of resurrection is involved), and the knitting together of nerves, muscles and tissues required is so complex that surgeons are only now, in the twenty-first century, beginning to achieve success with such grafting of limbs. But part of the shock, for the patient and his acquaintances, is that the new, functioning body part should be so completely foreign to the white man. When he starts to walk around, no one who sees him believes the miracle until they go to the graveyard and see for themselves that the dead Ethiopian now possesses a white leg, that there has been a straight swap.
To the original readers of this story, there could be nothing more foreign to white skin than black skin. Taken metaphorically rather than literally, the scene is about one’s sense of identity—not about limbs at all, but about a state of mind, about the splintering of the self. In the Caxton poem, the man has to wait a while before he is “wel come to hym self”: before he is fully awake perhaps, before he has “well come” to his senses. But also, before he is welcome; like “the man who fell out of bed,” he cannot rise until he accepts who he is.
How many owners of artificial limbs have felt something like this when their prostheses were first delivered? How alien must they feel to themselves? What happens to phantom limbs when they are usurped by wooden or metal pretenders to their position? While researching these issues, Oliver Sacks came across an interesting fact. Far from getting in the way of an artificial limb, a phantom limb turns out to be a prerequisite for wearing one. “All amputees,” Sacks wrote in his book The Man Who Mistook His Wife for a Hat, “and all who work with them, know that a phantom limb is essential if an artificial limb is to be used.” A fellow neurologist had written to Sacks that the phantom’s “value to the amputee is enormous. I am quite certain that no amputee with an artificial lower limb can walk on it satisfactorily until the body-image, in other words the phantom, is incorporated into it.” “Thus,” Sacks concluded, “the disappearance of a phantom may be disastrous, and its recovery, its reanimation, a matter of urgency. This may be effected in all sorts of ways. ... One such patient, under my care, describes how he must ‘wake up’ his phantom in the mornings: first he flexes the thigh-stump towards him, and then he slaps it sharply—‘like a baby’s bottom’—several times. On the fifth or sixth slap the phantom suddenly shoots forth, rekindled, fulgurated, by the peripheral stimulus. Only then can he put on his prosthesis and walk.”
Another of Sacks’s patients described the way in which his prosthetic limb helped with the pain in his phantom. “There’s this thing,” he said, “this ghost-foot, which sometimes hurts like hell—and the toes curl up, or go into spasm. This is worst at night, or with the prosthesis off, or when I’m not doing anything. It goes away when I strap the prosthesis on and walk. I still feel the leg then, vividly, but it’s a good phantom, different—it animates the prosthesis, and allows me to walk.”
The phantom, in other words, atrophies and causes pain without the prosthesis to give it purpose, and the prosthesis can only function when animated—literally given a soul, as Nelson would have it—by the phantom. The limb-wearer becomes a man-machine, given bionic life when “fulgurated” or “faradised,” like the monster in Mary Shelley’s Frankenstein.
The most recent research into phantom limbs, conducted by the American neurologist V. S. Ramachandran and popularized in his book Phantoms in the Brain, shows that the phenomenon may be connected to a sort of “artificial man” in the human brain. There is, on the brain’s surface, a map of the body in the awkward shape of a man. The map is known as “the Penfield homunculus.” In the homunculus, the hand and thumb are next to the face. When Ramachandran experimented with a phantom hand patient by lightly rubbing his cheek, the patient confirmed that he felt the rubbing in his missing hand. In other words, in cases of phantom limbs, the brain receives messages in a neighboring area, though that area is not, on the external human body, adjacent. Other patients confirmed this theory. For example, two people reported sensations in their phantom foot when they had sex, and were astonished to discover an explanation for this: in the brain, on the Penfield map, the genitals and the feet are next to each other. “I never suspected,” Ramachandran wryly concludes, “that I would begin seeking an explanation for phantom limbs and end up explaining foot fetishes as well.”
But Ramachandran also wanted to help his patients who had pain in their phantoms, or found them paralyzed, as Mitchell’s patients had, in the position in which they’d last felt them. He developed a novel technique for this, which involved giving the patient the impression that the phantom they felt but could not see was physically present. He constructed a “virtual reality box,” with a vertical mirror inside it and two holes in the front. He asked patients to put both arms through the holes and to move them about in tandem. With the mirror apparently reversing their arms, the patients saw their phantoms actually move. In some cases the paralysis ended; in others the phantoms disappeared altogether, along with the pain. What appeared to have been performed, as Ramachandran put it, was “the first example in medical history of a successful ‘amputation’ of a phantom limb.” “Philip,” he said of one of his patients, “seemed to think I was some kind of magician” and indeed the “virtual reality box” he invented is not unlike the cabinet tricks used by stage magicians in the nineteenth century. The doctor had cured a delusion using illusionism.
This article is published as part of Cabinet’s contribution to documenta 12 magazines, a collective worldwide editorial project linking over seventy print and online periodicals, as well as other media.
Gaby Wood is a New York–based author and a staff writer at the Observer, London. A version of her essay in this issue was originally published in The Phantom Museum (Profile Books, 2003).
Spotted an error? Email us at corrections at cabinetmagazine dot org.
If you’ve enjoyed the free articles that we offer on our site, please consider subscribing to our nonprofit magazine, which includes unlimited access to all our archives.